


Where Has All the Bird Flu Gone?
All quiet on the American front for H5N1, but not necessarily the good kind of quiet


All seems quiet on the H5N1 avian flu front. We haven’t had a new human case in months. Infected dairy herds and poultry farms aren’t leading news stories the way they were 6 months ago. Egg prices have dropped. Most people can be forgiven for thinking the danger has passed, particularly given this era of constant turmoil, in which being terrorized by existential threats has become ubiquitous. It’s understandable why the lack of information about the risk of H5N1 is a comfort to many.
I wish I could be reassured by the lack of new cases. Alas, I am cursed with excessive bird flu knowledge and first-hand experience with the American response to it. Right now, there is one thing standing between us and a flu pandemic: the H5N1 viruses that are circulating can infect people, but can’t be transmitted efficiently between them. They are, however, segmented RNA viruses, which means that they can rapidly change.
We know that it is possible for H5N1 to gain the ability to transmit between ferrets (which are very similar in respiratory physiology and virus receptor distribution) by the aerosol route. We also know that the barrier to this happening is pretty low, at least in ferrets. Influenza viruses, like all RNA viruses, have a high mutation rate and can adapt quickly to a new host. Flu genomes are divided into 8 pieces of RNA that be swapped or “reassorted” with other flu viruses. Mutation happens every time the virus copies its genome and reassortment can occur any time there is a co-infection. Every new case of infection increases the risk of a virus capable of human-to-human transmission emerging.
If this happens, preventing a pandemic will depend on rapidly detecting the first clusters of infected people so that they can be isolated. Contact tracing will need to occur immediately to prevent outward spread. Based on human case data so far, the H5N1 viruses circulating in the US cause disease severe enough to require medical intervention in about 6% of the people who are infected. Most of the human cases have had relatively mild symptoms: conjunctivitis (pink eye), minor respiratory symptoms, low fevers. If the virus begins spreading between people, it might not be noticed, since people who aren’t very sick don’t usually seek out medical care they don’t need. People who aren’t very sick do, however, usually continue working, socializing, and traveling. One infected person could spread the virus far and wide, seeding new outbreaks wherever they go. If we rely solely on symptoms or people who show up to the emergency room to detect new human cases, then by the time we recognize there are a bunch of H5N1 patients in a hospital, it will already be too late to contain.
To stop a possible H5N1 pandemic, we need to test for it. The problem is that we aren’t doing it.
No news is not good news
It seems pretty straightforward: if there are no positive tests, there’s no bird flu around, right? Well, yes, but only if you are actually testing. There’s mounting evidence that testing has declined precipitously.
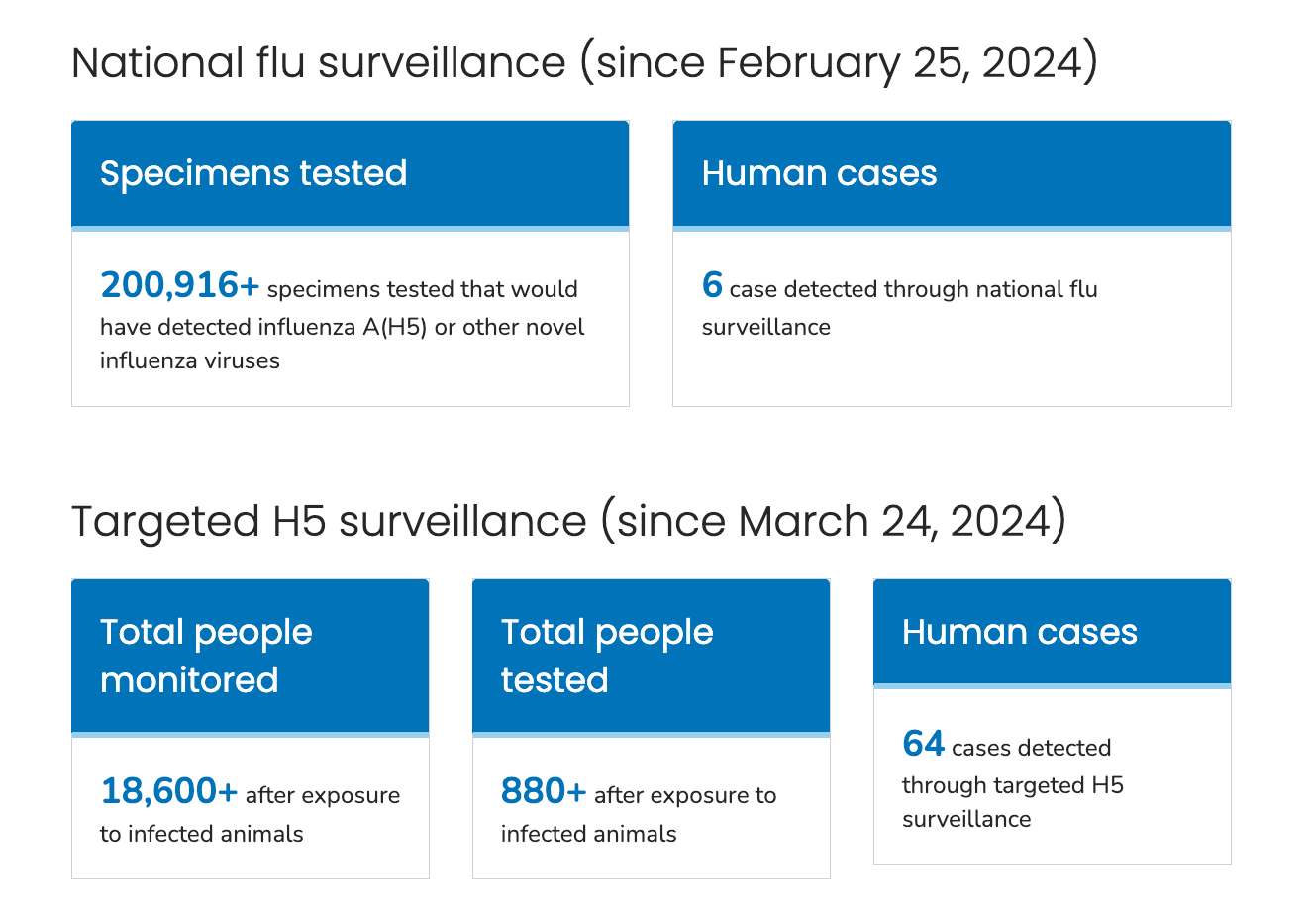
Influenza testing has always been patchy and surveillance has always been dependent on funding and available resources, both of which are now in short supply. However, last year, CDC detected 70 human cases in the US through a combination of 2 testing approaches. One is our National Influenza Surveillance System, which detected 6 of those cases. National flu surveillance is basically reporting the results of diagnostic tests from across the country. Sometimes this reporting can be delayed and it takes additional time to confirm an avian flu infection. That’s why out of more than 200,000 tests, only 6 cases were detected this way.
The majority of human cases were detected by targeted H5N1 surveillance, which is faster and more likely to identify cases since it is focused on people who are more likely to get infected. This involves symptom monitoring and testing people with a known exposure to an infected animal (usually in the context of a dairy or poultry farm, providing veterinary care, and a backyard flock). Because this type of testing seeks out people with higher exposure risk, it’s more likely to detect positive cases.
.
Animal testing is even harder to track in the US, since it’s not reported uniformly and the amount of testing that occurs varies wildly from state to state. This depends on all kinds of things: state and local agricultural and animal health policies and practices, funding for animal health, relationships with veterinarians, animal owners, and industry, surveillance activity, reporting requirements, geographical region, accessibility, environment, and the animal species in question. It’s pretty easy to tell if a turkey flock has H5N1 because the barn will go from what I assume is normally a relatively peaceful gobblefest into a neck twisting, bloody diarrhea-filled, screaming avian death explosion overnight. Eventually infected cows will be detected by farmers because they stop producing milk, although whether these cases are reported or not is another story. Most people would also notice if their pet cat died of horrible encephalitis, as many pets have by now. But how do you detect flu in pigs, which might get some mild respiratory symptoms from H5N1 if they even get sick at all? The answer is we generally don’t, because we aren’t doing surveillance testing in animals, even agriculturally critical species like pigs.
What we do know is that poultry outbreaks still occur. Dairy herds continue to test positive. Spillovers of H5N1 to humans is occurring in other parts of the world. Cambodia has had 12 bird-to-human cases this year. H5N1 is still circulating in wild birds. We’re still finding dead wildlife as well. Bird flu didn’t stop infecting new hosts. We just stopped looking for it.
First responders, worst responders
The US response to the avian flu outbreak has never been adequate. Throughout 2024 and up until the week before the inauguration, the CDC and USDA held ad hoc H5N1 Expert Briefings, where officials from the CDC and the USDA (and often FDA, BARDA, and ASPR) would update us on the situation. There were about 100 people invited to the briefing, including physicians, epidemiologists, public health officials, veterinarians, industry and agricultural scientists, vaccinologists, and virologists like me. Although I strongly suspect these meetings were partially intended to manage what we would all say to the press about our satisfaction with the government’s response, they were also great in a lot of ways. They provided us a forum to engage directly with the people leading the response in government and on the ground doing the work. We were able to ask questions, as well as give feedback on the responses. Even though many of us were quite critical of the H5N1 response under the Biden administration, I think most of us were grateful for the opportunity to exchange information with government officials.
There was a lot to criticize about the Biden response to the dairy cow outbreak just about testing. At the outset, the USDA was slow to share sequence data and even slower to share metadata that would allow scientists—specifically me and some of my colleagues—to link a virus with the farm where it came from and the time it was collected, tracing the spread of the epizootic (epidemic in animals) and scanning for the emergence of mutants associated with adaptation to humans or increased transmissibility. We were able to get this metadata from a sharp-eyed colleague who noticed that it was in a slide shown at a USDA webinar. As a result, we were able to show that the dairy cow outbreak began via a single spillover from bird to cow in Texas in late 2023, consistent with USDA’s own analysis. However, because these delays in sequence and metadata sharing have continued, it is not really possible to understand how many samples have been tested and where and when. We’ve never had a good understanding of the full scale of the cattle outbreak as a result.
The Biden-era CDC also did not earn any accolades for its response. As seems to be the CDC’s signature move, they screwed up developing a PCR test, which was a problem since CDC at the time was the only diagnostic lab in the country that could confirm human H5N1 cases. The CDC monopoly on diagnostic testing was a big problem in early 2020, too, when they made a COVID PCR test that didn’t work and failed to detect community transmission in the Seattle area for the entire month of February. What happened here was pretty simple: if your test doesn’t work, you can’t use it to detect cases. Although they did fix the CDC test and the US government contracted with private companies to expand access to diagnostic testing, CDC was very slow to ramp up testing or making it broadly accessible. Testing was only offered to people who tested positive for a non-seasonal subtype of influenza A or people who had a high-risk exposure (hit with a faceful of infected milk, depopulating a poultry farm, cuddled with sick backyard birds, etc) and were also symptomatic. By the time monitoring and targeted testing ramped up in mid-summer 2024, the number of human cases began to explode. Since then, other serological studies that look for antibodies as evidence of prior infection have indicated that there have been quite a few undetected cases. And, although they were faster to share sequence data publicly, CDC did not provide details about testing so it was difficult to ascertain what was happening when and where.
Nobody was really sure why everything was so delayed, although some—including myself—wondered if political pressures might explain it. The Democrats had made a very clear calculation that a pro-public health platform wasn’t going to be a winning campaign issue the way it was in 2020. The public had pandemic fatigue and science itself had become deeply polarizing and distorted by misinformation. Most people simply did not want to hear about yet another terrible virus maybe causing an even worse pandemic, but also maybe not. Slow-walking a response to H5N1 by specifically not trying too hard to detect H5N1-positive herds or new human cases associated with dairy or poultry production kept pandemics out of political discussions.
If this was intentional, I think it was more due to wishful thinking than cunning and political cynicism. The government officials who ran these meetings would routinely claim that we were on the verge of containing the cattle outbreak, which increasingly came across as desperately hopeful wishcasting rather than coldly calculated dishonesty. Based on the explanations offered in the briefings, it seemed like most of the delays were caused by a combination of territorialism and bureaucracy. The scientists at USDA and CDC were really collaborative and great to talk with, but their ability to share information was limited by agency data sharing policies. COVID trashed the existing playbooks for pandemic response, the cultural landscape had radically shifted, and nobody expected that avian influenza would infect cattle in the first place. There were complex relationship dynamics between the government, producers, and industry. Without a coherent response plan, these agencies were not structurally flexible or dynamic enough to respond effectively or urgently enough to meet the moment.
I remain grateful that the prior administration did hold these briefings, because even the half-assed response from 2024 seems like John Snow-level legendary outbreak response in comparison to what has happened under the Trump administration. The week before the inauguration, the final Expert Briefing was a somber affair, despite the CDC and USDA both announcing that testing was funded, in place, and being implemented. When we signed off, one of my academic colleagues on the call thanked the government officials who organized it for their openness and said that they hoped these briefings would continue. Every single government official who led their agency’s response in those briefings has since lost their job.
Gold Standard Doing Nothing
The avian flu response under Secretary of Agriculture Brooke Rollins and Secretary of Health and Human Services Robert F. Kennedy, Jr. is not a response at all. It mostly involves giving USDA a billion dollars to lower the price of eggs and letting Rollins and Kennedy float terrible ideas they claim represent “Gold Standard Science.”
I don’t know what constitutes “Gold Standard” virology or outbreak response since Trump and Kennedy just made it up, but as far as I can tell, it means doing nothing. Among the dreadful suggestions being bandied about is just letting H5N1 tear through poultry farms without culling the infected birds. According to Kennedy, surviving birds can go on to populate the earth with magically flu-resistant superchickens. Not only is this horrifically inhumane and incredibly dangerous to workers cleaning up the aftermath, it won’t work. H5N1 kills nearly all the birds that it infects. Any survivors aren’t going to be healthy enough to resume productive egg laying, much less bear an army of flu-impervious broilers. Letting the virus run its course will not select for super anything except perhaps more efficiently transmitted, pathogenic, or immune-evasive viruses. If they take another tip from Kennedy and start prophylactically dosing the birds with oseltamivir (Tamiflu), this will select for viruses that are resistant to our first line class of antiviral drugs. The “Let ‘Er Rip” plan for bird flu is a really, really bad idea that will have severe health, economic, agricultural, environmental, and food security consequences. Because this plan is to basically do nothing.
That’s reflected in the testing situation. I did a little analysis of how much testing has occurred since Trump took office by calculating the number of tests or cases monitored each month using archived versions of the CDC’s Bird Flu situation report. Overall, national surveillance testing is decreasing, although this will likely rise again in the fall for flu season, since this is based on any flu diagnostic test that gets run in the US. It’s not flu season right now, so there are fewer flu tests being run overall. However, the number of people who are being monitored after an exposure is reduced or staying relatively static each month, while the number of tests being performed on people being monitored dropping to almost nothing. For the past three months, no tests have evidently been performed as part of the targeted testing program.

There are several possible explanations for the decrease in targeted monitoring and testing. One is that there’s actually nobody getting exposed or testing positive for H5N1, although I think that’s unlikely. Another is that dairy and poultry workers are often immigrants from Central or South America, and thus less likely to report anything for fear of winding up in an ICE concentration camp. It is also possible that the numbers are waning seasonally, although there does not appear to be a seasonal component to the cattle outbreak.
But in my opinion, the most likely possibility is that we are seeing the desired results of Gold Standard doing nothing. Because we are doing nothing, we don’t know how much risk exists or not. And because there is no funding support for the essential research and surveillance we need to assess risk and do something to mitigate it, we won’t have the option of doing that. There won’t be anyone to do it due to job losses at CDC and USDA. An Executive Order banning broad categories of virology and epidemiology research will stall development of antiviral drugs and vaccines. The 10 million doses of H5N1 vaccine in the national stockpile are partially stored in 5 mL multidose vials containing the preservative thimerosal, which the Advisory Committee on Immunization Practices effectively banned at their most recent meeting. Local hospitals and public offices will close from the combined effect of withdrawn federal grant funds and the One Big Beautiful Bill that destroyed a big chunk of our national health infrastructure. If H5N1 does “go pandemic,” we are well and truly cooked.
H5N1, being a virus, doesn’t care about any of this. It’s continuing its usual agenda of virus business: infecting new hosts, replicating, adapting, spreading. Gold Standard doing nothing is very compatible with allowing H5N1 to establish itself in various mammalian hosts nationwide. Right in time for flu season, when suddenly H5N1 will have new human-adapted influenza viruses circulating that it can reassort with. And if H5N1 does gain the ability to spread between people and isn’t detected or contained, the pandemic that will result will make us yearn for COVID.
But just because H5N1 is quiet doesn’t mean that we have to be, nor do we need to adhere to the Gold Standard of maliciously negligent inaction. Everyone should be concerned about the pandemic risk that the destruction of our national capacity to infectious disease threats presents. We must unite against this administration’s attacks on American health, science, agriculture, food security, and the economy. We should make some noise before bird flu gets a chance to do so.
Thank you for this review of the recent history of H5N1. Ventana Wildlife Society is vaccinating condors against H5N1, https://www.ventanaws.org/condorthreats.html,
after several deaths in Arizona. https://www.fws.gov/program/california-condor-recovery/southwest-california-condor-flock-hpai-information-updates-2023. H5N1 devastated Southern Elephant Seals in 2024, https://www.vetmed.ucdavis.edu/news/catastrophic-mortality-elephant-seals-argentina-identified-outbreak-avian-influenza, raising concerns for the Northern Elephant Seals along the California coast. The Southern seals appear to be recovering, https://www.thecooldown.com/outdoors/elephant-seal-population-recovery-chile-avian-flu/. Could a seal vaccine be developed, an aerosol that could be administered by drone over seals on the beach?
While the Biden administration’s, and the medical community’s, responses to H5N1 may have been less than perfect, Biden’s appeal to compare him not to the Almighty, but to the alternative, seems more vivid now than it was during the campaign.
Thanks for providing this information to the public, Dr. Rasmussen.