
Evidence-Based ACIP is So Back
Never underestimate vaccinologists with a standardized framework for interpreting evidence

It’s been a bad year for the Advisory Committee for Immunization Practices (ACIP), an independent, unpaid expert panel that evaluates evidence about vaccines, makes evidence-based recommendations for their use, and decides vaccination policies in a democratic and data-driven way. These recommendations are central to determining vaccine access, and are used by the Centers for Medicare and Medicaid Services (CMS) to decide coverage, insurers to determine claim reimbursements, and the CDC’s Vaccines for Children (VFC) program to provide more than 50% of all scheduled childhood vaccinations to American kids.

However, US Secretary of Health and Human Services (HHS) Robert F. Kennedy, Jr. is a complete weirdo about children and hates vaccines to the core of his creepy, corrupted soul. He is also a skilled litigator who specializes in using propaganda and shrewd bureaucratic manipulation to create policies that strip people of access to vaccination. So he set ACIP in his sights as a primary weapon in his fight to kill kids with preventable diseases.
In June, Kennedy fired all 17 members of the ACIP and replaced them with a viper’s nest of anti-vax quacks with minimal scientific qualifications or policymaking experience and extensive financial conflicts of interest. Kennedy also booted the ACIP liaisons (experts from scientific and medical professional societies who don’t vote but advise on evidence) from workgroups convened to develop evidence packages for ACIP to review. Kennedy fired CDC Director Susan Monarez in late August for refusing to rubber stamp evidence-free ACIP recommendations, triggering the principled resignations of National Center for Immunization and Respiratory Diseases (NCIRD) Director Demetre Daskalakis, National Center for Emerging Zoonotic and Infectious Diseases (NCEZID) Daniel Jernigan, and Chief Medical Officer Debra Houry.
The new ACIP immediately began their assigned task of dismantling vaccine accessibility. They derecommended vaccines containing thimerosal at their June meeting and signaled their intent to deschedule the measles-mumps-rubella-varicella (MMRV) combination vaccine. They made good on that promise at their September meeting. They also tried to do the same to the hepatitis B virus (HBV) vaccine and COVID-19 vaccines, but their incompetence prevented them from making coherent recommendations. They are not yet so emboldened as to just vote on “we recommend shitcanning as many vaccines as possible,” though that is their ultimate goal. Instead they called it “individual decision-making” and framed it as a triumphant strike against the dogmatic and venal status quo.
“Informed consent is back,” crowed Acting CDC Director Jim O’Neill. I can’t fault him completely for not knowing that informed consent is actually still here, since ACIP never recommended that people be vaccinated without their knowledge or against their will. O’Neill, like the ACIP he oversees, is grossly unqualified to direct national public health policy. His sole experience is investing in longevity and anti-aging businesses and worked in a number of executive roles for eschatological psychopath and billionaire AI surveillance state mogul Peter Thiel. He previously supported commercializing human organs and thinks that FDA should not regulate any lab test that uses an algorithm, like genetic testing. Under his hapless libertarian stewardship, the CDC continues its acceleration towards complete and total demolition.
The chaos at CDC is certainly exacerbated by the malfeasant bumbling of the current ACIP membership. It is difficult to accurately forecast the damage it will cause due to the overwhelming scale and scope of the maelstrom engulfing vaccine policy and public health. Fortunately, there are people who can help. There is a group of people who are experts at using standardized frameworks to evaluate evidence in a reliable and consistent way: the former members of ACIP.
So that’s exactly what they did. A cohort of fired ACIP members conducted a rigorous analysis of how their replacements are doing at their old jobs and published it yesterday in Vaccine. There’s nothing I enjoy more than reading a scathing evidence-based takedown, especially in an academic journal and especially when it contains glorious paragraphs like the one below, so time for another journal club!
Standardized frameworks are back
What I really love about this paper is that it is ACIP doing what it did best before being usurped by conspiracy-addled lunatics: using a rigorous and standardized method for assessing evidence. Historically, ACIP would develop policy questions by examining the key populations/problems, interventions, comparisons, and outcomes (PICO). They used two frameworks for making evidence-based policy recommendations: one called Grading of Recommendations, Assessment, Development, and Evaluation (GRADE) to analyze evidence and another called Evidence-to-Recommendations (EtR) to develop recommendations based on this analysis.
In this paper, Asturias et al used the same approach to standardized evidence review using a different tool for evaluating the maturity of national immunization technical advisory groups (NITAG). The NITAG Maturity Assessment Tool is basically a standardized performance review that applies a scoring rubric across 7 different indicators of advisory group maturity. Within each indicator is a series of criteria assigned to a specific level of maturity. For example, the “Independence and Non-Bias” indicator rates different levels of stringency with conflict of interest disclosures, transparency, and independence as a series of increasingly mature categories, from Basic to Leading Edge.
Asturias et al applied this tool to compare the maturity status of ACIP at the time of their last meeting in April 2025 and with the current panel after their last meeting in September. Uh oh…the new ACIP’s performance has declined significantly across every indicator category compared to their predecessors.

They scored especially low in the Independence and Non-Bias, Making Recommendations, Integration into Policy Making, and Stakeholder Recognition indicators. This is because they are extremely biased and conflicted, their recommendations lacked evidentiary support and were in many cases not actionable or within ACIP’s scope of authority (such as their attempt to require prescriptions for COVID-19 vaccines), they were so inept that they were unable to even make recommendations about the HBV vaccine, and they ignored or outright attacked any critical stakeholders who disagreed with them.
This demonstrable decline in performance quality would be embarrassing to most vaccine experts with even the slightest concern for professional credibility; however, that assumes they have the capacity for shame and remorse. ACIP Chair Martin Kulldorff once posted a picture of a guillotine to illustrate his contempt for critics of the mass infection policy he proposed with now-NIH Director Jay Bhattacharya. Shortly after a domestic terrorist who believed he suffered a vaccine injury shot more than 500 rounds at CDC and killed a police officer, ACIP member Robert Malone posted gun memes on his Substack so tasteless that Senator Richard Blumenthal demanded he be fired. Malone clapped back with the old excuse that he was just joking and trying to stir up status quo-disrupting discourse, and further bemoaned that he is also a victim of “woke censorship tactics” and confirmed with Grok that this is illegal. Malone wasn’t too put off and has since given explicitly anti-vax webinars with ACIP member and COVID-19 workgroup chair Retsef Levi. Levi has been claiming since 2023 that mRNA vaccines are deadly and should be banned. He is so unqualified that HHS lawyers questioned the legality of his appointment to workgroup chair, given it expanded his power to unilaterally decide vaccine policy. ACIP member Vicky Pebsworth has spent decades testifying in state courts against vaccines and led an organization dedicated to spreading anti-vax propaganda. Newer additions to the ACIP include more anti-vaxxers from the “medical freedom” contingent of the movement such as prophet of sudden infant death syndrome and adolescent myocarditis doom Kirk Milhoan, school immunization opponent Evelyn Griffin, and COVID death underestimator Catherine Stein. New ACIP wears their opposition to vaccines like a badge of honor. They are not ashamed of their lies.
The inept pseudoscientific rot in the current ACIP runs deep, and this was apparent in their voting record at the last ACIP meeting. Asturias et al itemized whether or not the panel adhered to standard ACIP practices on the votes for three vaccines: de-recommending the MMRV (successful, with caveats), de-recommending the birth dose of HBV (unsuccessful), and restricting COVID-19 access (mostly unsuccessful). Unsurprisingly, they did not.
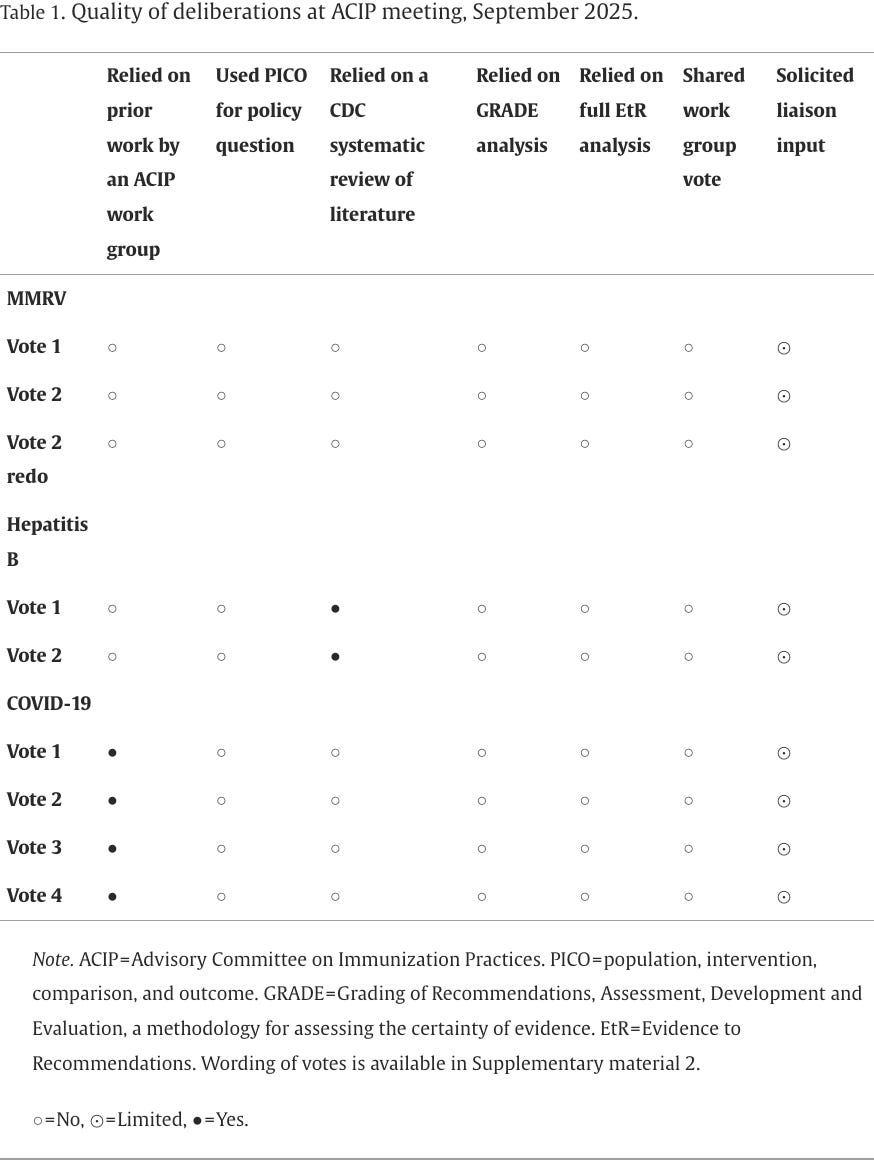
The ACIP did not formulate questions using PICO or examine the evidence using the GRADE or EtR frameworks for any of the votes. While they did rely on Levi’s COVID-19 workgroup report, it included entire unsupported sections about turbo cancer, a grossly underpowered genome-wide association study on myocarditis, and grounding the discussion in the false pretense that vaccine injuries and mortality are vastly underreported. They also relied on a CDC systematic literature review during their deliberations on HBV, which is probably why they were unable to actually pass any of their recommendations to deprive babies of protection against a virus that causes chronic infection and liver cancer. However, none of the normal processes in place for creating standardized, broadly applicable, effective recommendations occurred for any of the votes. This is an unacceptable deviation from the prior practice and will cause significant harm in the form of vaccine policy that results in reduced vaccination.
Asturias et al reasonably conclude that ACIP’s measurable performance decline and potential impacts are due to the following four factors:
Misplaced focus and reductions in choice and access: ACIP is focusing on unimportant issues (like febrile seizures) and making unsupported recommendations that interfere with people accessing vaccines (like MMRV and multi-dose flu vaccines containing thimerosal). Already these have reduced vaccine access. In the case of the MMRV, their ineptitude at policymaking further complicated things when they voted on recommendations that made it unclear if the recommendation impacted programs like VFC or not and they had to revote. Also, by wasting two entire ACIP meetings on imaginary harms associated with vaccines that have been used safely for years or decades, ACIP has neglected other, completely new vaccines in development for cytomegalovirus (CMV) and Lyme disease, monitoring RSV immunization safety and effectiveness, and assessing whether the HPV vaccine can be given to kids as a single dose.
Inconsistent processes and low-quality research data: Levi’s specialty is posing ludicrous hypotheses (“COVID vaccines kill people”) or appealing to ignorance about theoretical harms (“we can never know if people who had a febrile seizure as a baby have a lifelong vaccine injury”) and then selectively cherry-picking or manipulating underpowered, unevaluated, or anecdotal evidence to invent or exaggerate vaccine injuries. This approach appears to be practiced by the majority of the new ACIP. It provides a mechanism for fabricating evidence to support descheduling any vaccine they like.
Limited expertise in vaccinology and clinical practice: For a panel that is intended to make expert recommendations for the clinical use of vaccines, ACIP is mostly devoid of specific expertise in vaccine science and experience with immunization in practice. Pediatrician Cody Meissner is the only member of ACIP with any relevant qualifications and professional credibility in this regard. The current ACIP is populated by anti-vaxxers and medical contrarians who have made repeated false statements about immunization with no experience developing public health policies applicable to the entire diverse American population. Many have separate ties to Kennedy and anti-vax organizations like Children’s Health Defense, the Informed Consent Action Network, the Brownstone Institute, and Natural News. They know nothing about vaccines except how to lie about them.
Lack of transparency and loss of independence: ACIP has not published their meeting materials in a timely manner. Meeting agendas are not determined by public health needs and are designed to validate a predetermined conclusion: vaccines are unsafe and don’t work. Therefore, vaccination should be limited as much as possible. New ACIP members don’t comprehensively declare conflicts of interest. Most workgroups have been shut down and the ones that exist are, like Levi’s COVID-19 workgroup, under the complete control of their outrageously biased chair. This will ultimately further erode public trust and lead to vast health inequities along socioeconomic and geopolitical lines.
I have to agree with the authors that this bodes extremely poorly for vaccine policy in the US. The combined incompetence, malice, and dishonesty of the new ACIP and their methods, the poor quality of the data they manipulate to advance their goals, their hostility toward vaccines and public health, and their lack of transparency and ideological loyalty to the current anti-vax regime are going to put millions of Americans at risk for preventable diseases.
Feckless and reckless
It’s not clear when ACIP will meet again. They were supposed to meet today. However, the entire ACIP Secretariat was fired two weeks ago in the CDC Friday Night Shutdown Massacre. Although (I think) they were reinstated, the government shutdown continues with no end in sight. However, Asturias et al give a stark warning about what kind of policy recommendations we can expect from the new ACIP once they finally reconvene.
At their next meeting, I suspect ACIP will take another swing at HBV vaccines, potentially with a different angle. HBV vaccines contain aluminum salt adjuvants, which are squarely in Kennedy’s crosshairs. If ACIP is able to deschedule vaccines containing these adjuvants, it will affect many other vaccines as well, including hepatitis A virus (HAV), diphtheria, tetanus, pertussis, human papillomavirus (HPV), Haemophilus influenzae B (Hib), pneumococcal conjugates, meningococcal A and B, Japanese encephalitis virus (JEV), and some formulations of the polio vaccine. I also suspect that ACIP will target the MMR vaccine itself, claiming that the risk of febrile seizure is too high and offering monovalent alternatives that don’t exist and never will. I don’t think they are finished with COVID-19 or flu vaccines, either.
One tactic that has been employed by this administration is cutting such a broad swath of destruction through public health that the damage can’t be accurately measured. For all of Kennedy’s talk about “Gold Standard Science,” in practice the “Gold Standard” is no standards at all, based on the ACIP’s performance thus far. Fortunately, ACIP’s former high standards were well-defined, and Kennedy has not been able to memory-hole them just yet. They can still be applied and we can at least measure the impact of the devastation that new ACIP is inflicting on Americans.
In quantifying the vast deficiencies of their replacements, the former members of ACIP have once again demonstrated their commitment to evidence-based policymaking and scientific integrity. I grieve for their lost expertise, because their measurable insufficiency and extremist anti-public health agenda will lead to greater sorrow down the road from the preventable diseases that are already roaring back to life in our children and our elders. If we are to have any hope of recovering in the future, we must know in detail what we lost, how we lost it, and who was responsible. The only way to do that is by following the evidence while adhering to fundamental scientific and ethical principles. Although the outlook is grim, I am grateful to Asturias et al for continuing their service to transparently advance the interests of the American people.
Competing Interest Disclosure
I am the co-Editor-in-Chief of Vaccine and I was the editor who handled this paper, since the presubmission inquiry was made to me. My editorial decision to accept the manuscript was based on the recommendations of multiple non-conflicted peer reviewers selected based on expertise with vaccinology and vaccine policy and not my own assessment beyond my determination that it was within the aims and scope of Vaccine and was appropriate to send for peer review.
Somehow it slips my mind that he is a”skilled litigator”, as so many foolish and dangerous things come out of his mouth and department.
"Limited expertise in vaccinology and clinical practice"... That is accurate, if "limited" means expertise rated in the negative numbers.